
Check out this web site is about BCM:
Blue Cone Monochromacy
Created and supported by ‘BCM Families Foundation’.
Blue Cone Monochromat (BCM)
Congenital achromatopsia consists of two major forms, Rod monochromatism and Blue cone monochromatism. BCM is the rarer form of achromatopsia and nearly exclusively in males. Blue cone monochromatism, (BCM), also known as X-linked incomplete achromatopsia, was initially described by Blackwell and Blackwell in 1957.
Blackwell HR, Blackwell OM 1957 Blue mono-cone
monochromacy: a new color vision defect.
J Optical Soc America 47:338–341).
View our movie below, which provides an introduction to blue cone monochromatism.
It is an incomplete form of achromatopsia that presents with similar symptoms to rod monochromatism including light aversion, nystagmus, severe but incomplete color blindness and impaired visual acuity. It belongs to the group of stationary cone dysfunction syndromes that includes rod monochromatism. However, it has a completely different form of inheritance than rod monochromatism.
Incidence: The incidence of BCM is between 1 in 50,000 to 1 in 100,000 in males. BCM is a condition that occurs almost exclusively in males, but can technically occur in females. The incidence is so low in females that it may occur only 1 in 10 billion births.
As we see below, the normal retina has rods that see only black, white, and shades of grey and tones and three forms of color cones, red, green, and blue.
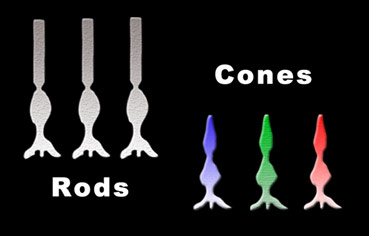
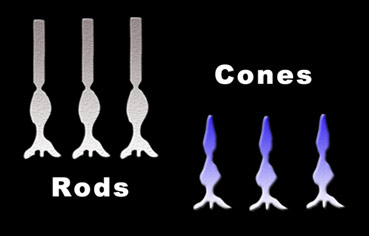
Patients with BCM have a failure of the red (L-cones ) and green (M-cones) owing to a failure of the specific photopigments to form. Thus blue cone monochromats, are left with only rods and the blue (S-cones).
Hemeralopia: Individuals with BCM experience hemeralopa or day blindness. It is a severe aversion to light that affects both those with BCM and rod monochromatism.The red, green, and blue cones have chemicals that are stable in bright light and thus allow us to see in bright light. The BCM individual has only the blue cones and rods available to function in bright light. Some with BCM may be less photophobic owing to the blue cones still functioning. Blue cones, however, account for only 2% of the total cones in the retina. Thus 98% of the total cones are not functioning. BCM individuals can still be overwhelmed by in bright light to the point of reducing their vision. They often learn to squint constantly in bright light and may require dark sunfilters inside and out.

Color Vision: Blue cone monochromats have only rods photoreceptors and blue cones receptors. They lack the photopigments in the red and the green cones. They have only one color channel functioning, the blue channel. Patients may report that they see blue or certain shades of blue and occasionally yellow. This does not mean that they see blue as you and I do.
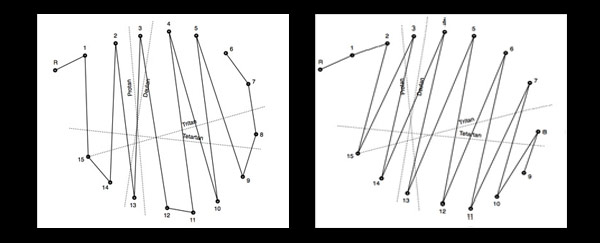
It may be possible to differentiate some blue cone monochromats from rod monochromats by the protan-like arrangement of the color disks on the D-15 or FM 100 Hue Test. However, not all blue cone monochromats behave in this manner. Some may perform like the rod monochromat on these tests.
The Mollon–Reffin (MR) Minimal test can help in the diagnosis of BCM. BCM males fail the protan and deutan axes, but retained discrimination on the tritan axis.
The Berson Test can differentiate Rod monochromats from BCM but not from progressive cone dystrophies. The Berson Test, however, has become difficult to acquire. On a HHR test the yellow blue axis may still be present, but lost in rod monochromats.
The D-15 test demonstrates the typical protan-like results demonstrated in many blue cone monochromats The right chart below shows the typical rod monochromat, while the left chart shows the typical findings of a blue cone monochromat on the D-15 Color Test.
Visual Acuity: The visual acuity of BCM individuals as a group averages slightly better than rod monochromats. The typical range is from 20/60 to 20/120, but we see cases at 20/200. Testing of visual acuity can vary dramatically based on the brightness of the room and acuity chart.
Refractive Error: While rod monochromats have a high incidence of hyperopia, BCM as a group shows high amounts of myopia. Refractive error can include hyperopia, astigmatism and myopia.
Nystagmus: Nystagmus is usually present from about three to six months of age. Cases have been reported without nystagmus. It is usually pendular and as in other achromats, may decrease with age.
Lack of Pupil Reflex Abnormalities: Paradoxical pupillary constriction in dim light frequently which is well established in many rod monochromatism appears to be much rareror in BCM.
Driving: BCM individuals with better visual acuity may be able to obtain a standard or restricted driver’s license if glare is properly controlled. Many are able to drive with bioptic systems.
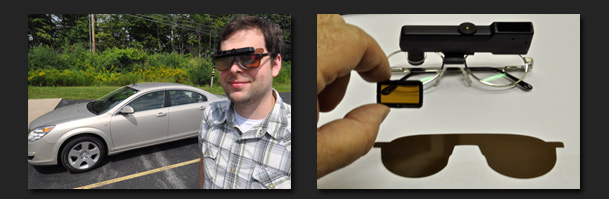
Filters: Magenta filters that are made from both red and blue dyes function well for those with BCM.
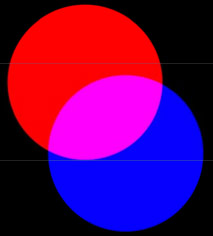
Solid dark red filters that are very effective for rod monochromats, unfortunately block the blue light and would thus cause a loss of the BCM individuals remaining blue channel. However, red lights reduce the energy reaching the rods thus allowing them to function at higher levels than normal. Blue light can activate the remaining blue cones in the retina aiding the patient's vision, however blue light is a very high energy light and can bleach out the rod photopigments. The answer is to combine both blue and red dyes into a magenta filter.

Magenta allows both the blue and red light to pass through to the retina. The red light helps the rod function while the blue activates the vblue cones. We can demonstrate this effect with a simple red/magenta flipper bar.
 The patient may report that the red filter suddenly reduces their vision while the magnenta filter may suddenly improve the vision. We can provide the magenta filter in either contact lenses or eyewear. The wrong color in the eyeglasses or contact lens can block the blue channel that the patient depends upon.
The patient may report that the red filter suddenly reduces their vision while the magnenta filter may suddenly improve the vision. We can provide the magenta filter in either contact lenses or eyewear. The wrong color in the eyeglasses or contact lens can block the blue channel that the patient depends upon.
Diagnosis: The presence from the first six months of life an aversion to the light, squinting, and nystagmus may lead to suspicion of achromatopsia. The family history of X-linked inheritance is a strong indicator of BCM. Establishing color vision loss further adds to the diagnosis. ERG testing can demonstrate loss of cone function with retained rod function.
To differentiate BCM from rod monochromats, color vision testing with the HHR, D-15 or 100 Hue tests may be helpful. Family history of X linked inheritance pattern and electrophysiological testing can aid in the diagnosis.
BCM individuals can be distinguished from rod monochromatism (RM) by psychophysical and electrophysiological testing. Although the photopic ERG is profoundly reduced in both, the S cone ERG is well preserved in BCM.
BCM must be differentiated from progressive cone dystrophies.