
The Low Vision of Achromatopsia
"When I was growing up, I was often treated as if I were blind and sometimes even called ‘that blind girl.’ I knew that not only was I definitely not blind, but I was a very visually oriented person. I knew that, in fact, I had a great deal of vision in the right kind of lighting."
- Member Achromatopsia Network
We can think of the visual acuity loss in achromatopsia as composed of two components, a variable transient component caused by debilitating glare whenever in bright light and the underlying physical visual acuity loss that remains when the light is controlled. In the graphic in the top banner of this page, we see the left side of the test chart overexposed causing vision to decrease. When the brightness of the right side of the chart is decreased, smaller letters can be read. The bright light induced vision loss is severe, but 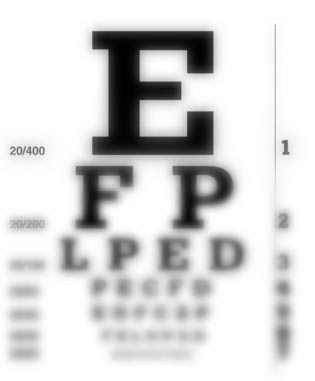 transitory depending on the light exposure. The underlying loss, after we control glare is quite manageable with simple low vision care.
transitory depending on the light exposure. The underlying loss, after we control glare is quite manageable with simple low vision care.
The visual acuity chart to the right shows the range of vision of the typical rod monochromat.
In rod monochromatism patients with glare controlled, the vision is
usually in the 20/100 to 20/200 range. In Blue Cone Monochromatism with the glare controlled, many patient will have better vision, sometimes as good as 20/60 but a few may be as low as 20/200. If light is not reduced with filters, the visual acuity can drop to profound loss in bright sunlight with either form of achromatopsia.
The Misconceptions of Legal Blindness
Though most achromats may be "legally blind", this is just a line on a chart drawn by the adoption of the 1936 Social Security Act. It was just a spot to begin providing additional services. Legal blindness, unfortunately, has become a label that may biase how other see the achromat. A legally blind achromat can function well in the world with appropriate filters and low vision aids.
Rachel Scodoris said it well in her book No End in Sight.
“Some people try to put limitations on me because they
want me to fit into the legal blind box.”
Rachel Scdoris, Dog Sled Racer, No End in Sight
by Rachel Scdoris and Rick Steber
The Cause of Decreased Vision
The underlying loss of acuity is primarily related to the loss of cone cell function in the macula of the retina where our best vision is normally achieved. Cone cells occur throughout the retina, but are are normally highly concentrated in the fovea, at the very center our retina.
Here, we see a photograph of the central retina of a "normal" on the left side and a young patient with achromatopsia on the right side.

Notice there is no significant difference in the normal and achromat retinas above by our gross observation. Thus diagnosis cannot be made by the appearance of the retina alone.
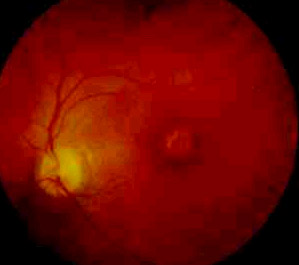
In older patients, some may show a "bulls eye" circle of pigmentation as shown in the retinal image to the right.
The fovea, the center of our macula, is our area of sharpest clearest vision. The cone cells are packed tightly into this tiny area to create a small zone of very high resolution vision. To see sharp and clear, we must aim the fovea at what we want to see. Below is a scan of the macular region and at the center, the fovea. Only in this area in a normal retina are the cones so compacted that the resolution is high enough to see 20/20.
The OCT Photoreceptor Integrity Line
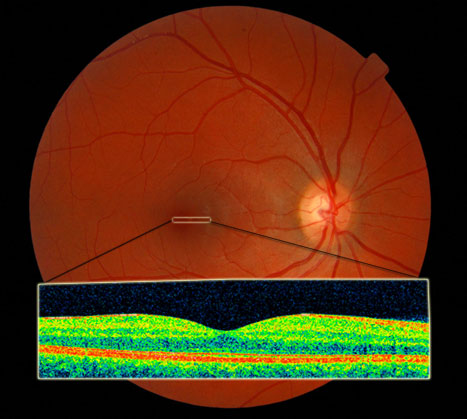
Above we see the Optical Coherence Tomography (OCT) Scan of a "normal" macula/foveal region of the retina.
In complete achromatopsia, however, the cone cells are either missing or not functioning throughout the retina. Since the fovea, the center of the macula, normally contains only red and green cones, we can look there to help confirm the loss or disruption of the cones in the retina. A new type of scanner, the Cirrus Optical Coherence Tomography (OCT) scanner allows us to scan this region.
we can look there to help confirm the loss or disruption of the cones in the retina. A new type of scanner, the Cirrus Optical Coherence Tomography (OCT) scanner allows us to scan this region.
The scan through the retina shows a line representative of photoreceptors created by the junction of the inner and outer segment of the rods and cone receptors. Loss of this line within the fovea where there are only (red and green) cone cells confirm a loss of red and green cone functioning.
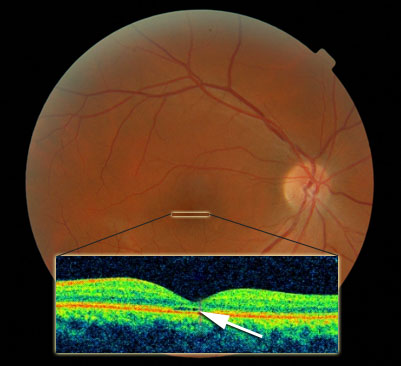
Note in the scan above the signal is missing in the fovea, an area where only cones should exist. The cones may be missing or malformed. This results in the need to use other parts of the retina, which do not have as sharp a resolution and thus reduced visual acuity.
Nystagmus may also further decrease vision. The more the eye moves the less stable time the image is on the area of the retina used by the patient. An increase in nystagmus may result in a direct temporary decrease in vision.
First Control the Light - Then Low Vision Care
In our practice, we have learned that the first step is to control the light and glare. Much of the information on this website features approaches we have developed to better control the debilitating glare. When possible, the filtered (red, amber-brown or magenta) contact lenses combined with sun wear has been the most successful. Once glare is controlled, we can consider a variety of low vision aids to help the patient. With glare controlled, low vision care becomes much easier.
See our section on low vision aids.